Student's Notes
Muhammad Na'im is presently in Year 4 Medicine. USM. He will enter Year 5 in July 2010 and hopes to graduate by May 2011.
http://jacknaimsnotes.blogspot.com/2009/03/blood-in-urine.html
Tuesday, 29 December 2009
Observation of Urine
Visual Inspection of Urine / Urine Appearance
Normal, fresh urine is clear and pale to dark yellow or amber in color. Cloudiness may be caused by excessive cellular material or protein in the urine or may reflect from crystallization or precipitation of salts upon standing at room temperature or in the refrigerator. Clearing of the specimen after addition of a small amount of acid indicates that precipitation of salts is the probable cause of tubidity. A red or reddish-brown color could be from a food dye, consumption of beets, a drug, or the presence of either hemoglobin (from the breakdown of blood) or myoglobin (muscle breakdown). If the sample contains many red blood cells, it would be cloudy as well as red.
http://www.medical-library.net/urinalysis_interpretation.html
Normal, fresh urine is clear and pale to dark yellow or amber in color. Cloudiness may be caused by excessive cellular material or protein in the urine or may reflect from crystallization or precipitation of salts upon standing at room temperature or in the refrigerator. Clearing of the specimen after addition of a small amount of acid indicates that precipitation of salts is the probable cause of tubidity. A red or reddish-brown color could be from a food dye, consumption of beets, a drug, or the presence of either hemoglobin (from the breakdown of blood) or myoglobin (muscle breakdown). If the sample contains many red blood cells, it would be cloudy as well as red.
http://www.medical-library.net/urinalysis_interpretation.html
Urine FEME
FEME stands for Full Examination, Microscopic Examination. Urine FEME is also referred to as Microscopic Urinalysis.




How is it done?
A sample of well-mixed urine (usually 10-15 ml) is centrifuged in a test tube at relatively low speed (about 2000-3,000 rpm) for 5-10 minutes which produces a concentration of sediment (cellular matter) at the bottom of the tube.
The fluid on top is poured off to a volume of 0.2 ml to 0.5 ml left inside the tube.
The sediment is resuspended in the remaining urine by flicking the bottom of the tube several times.
A drop of resuspended sediment is poured onto a glass slide and a thin slice of glass (a coverslip) is placed over it.
The sediment is first examined under low power to identify crystals, casts, squamous cells, and other large objects.
"Casts" are plugs of material which came from individual tubules.
The number of casts seen are usually reported as number of each type found per low power field (LPF).
For an example: "5-10 hyaline casts/LPF."
Since the number of elements found in each field may vary considerably from one field to the next, several fields are averaged.
Then, examination is carried out at high power to identify crystals, cells, and bacteria.
The various types of cells are usually described as the number of each type found per average high power field (HPF).
For example: "1-5 WBC/HPF."
External link
http://www.medical-library.net/urinalysis_interpretation.html
Urine Dipstick Test
Reading The Dipstick
The dipstick yields valuable information which is available by direct observation of the coloured patches on the test strip (dipstick) after brief immersion in the urine specimen. There are a number of parameters which are determined: pH, specific gravity (S.G.), protein, glucose, ketones, nitrite and leukocyte esterase.
Acid/Base (pH)
The dipstick yields the pH, a reflection of acid/base levels. The initial filtrate of blood plasma is usually acidified by the renal tubules and collecting ducts (microscopic structures in the kidneys of which there are millions) from a pH of 7.4 to about 6 in the final urine. in other words, the urine is acidified. However, depending on the acid-base status, urinary pH may range from as low as 4.5 to as high as 8.0. One task nature has assigned to the kidneys is to rid the body of acid.
Specific Gravity (S.G.)
Specific gravity measures urine density which reflects the ability of the kidney to concentrate or dilute the urine relative to the plasma from which it is filtered. Although dipsticks are available that also measure specific gravity in approximations, most laboratories measure specific gravity with a instrument call a refractometer. Specific gravity between 1.002 and 1.035 on a random sample should be considered normal if kidney function is normal. Any measurement below 1.007 to 1.010 indicates hydration and any measurement above it indicates relative dehydration. Urine having a specific gravity over 1.035 is either contaminated, contains very high levels of glucose, or the patient may have recently received high density radiopaque dyes intravenously for radiographic studies or low molecular weight dextran solutions.
Protein
While the dipstick test has a portein measurement, more elaborate tests for urine protein should be performed since cells suspended in normal urine can produce a false high estimation of protein. Normal total protein excretion does not usually exceed 150 mg/24 hours or 10 mg/100 ml in any single specimen. More than 150 mg/day is considered proteinuria. Proteinuria greater than 3.5 gm/24 hours is severe and indicates the nephrotic syndrome. Dipsticks detect protein by production of color with an indicator dye, Bromphenol blue, which is most sensitive to albumin but detects globulins and Bence-Jones protein poorly. Precipitation by heat is a better semiquantitative method, but overall, it is not a highly sensitive test. The sulfosalicylic acid test is a more sensitive precipitation test. It can detect albumin, globulins, and Bence-Jones protein at low concentrations. "Trace" protein is equivalent to 10 mg/100 ml or about 150 mg/24 hours (the upper limit of normal). 1+ corresponds to about 200-500 mg/24 hours; 2+ to 0.5-1.5 gm/24 hours, a 3+ to 2-5 gm/24 hours, and a 4+ represents 7 gm/24 hours or greater.
Glucose
Glycosuria (excess sugar in urine) generally means diabetes mellitus.
Ketones
Ketones (acetone, aceotacetic acid, beta-hydroxybutyric acid) may be present in diabetic ketosis or other forms of calorie deprivation (e.g. starvation). Ketones are easily detected using either dipsticks or test tablets containing sodium nitroprusside.
Nitrite
A positive nitrite test indicates that bacteria may be present in significant numbers. Gram negative rods such as E. coli are more likely to give a positive test.
Leukocyte Esterase
A positive leukocyte esterase test results from the presence of white blood cells either as whole cells or as destroyed cells. A negative leukocyte esterase test means that an infection is unlikely. Without additional evidence there is no need for culture.
http://www.medical-library.net/urinalysis_interpretation.html
The dipstick yields valuable information which is available by direct observation of the coloured patches on the test strip (dipstick) after brief immersion in the urine specimen. There are a number of parameters which are determined: pH, specific gravity (S.G.), protein, glucose, ketones, nitrite and leukocyte esterase.
Acid/Base (pH)
The dipstick yields the pH, a reflection of acid/base levels. The initial filtrate of blood plasma is usually acidified by the renal tubules and collecting ducts (microscopic structures in the kidneys of which there are millions) from a pH of 7.4 to about 6 in the final urine. in other words, the urine is acidified. However, depending on the acid-base status, urinary pH may range from as low as 4.5 to as high as 8.0. One task nature has assigned to the kidneys is to rid the body of acid.
Specific Gravity (S.G.)
Specific gravity measures urine density which reflects the ability of the kidney to concentrate or dilute the urine relative to the plasma from which it is filtered. Although dipsticks are available that also measure specific gravity in approximations, most laboratories measure specific gravity with a instrument call a refractometer. Specific gravity between 1.002 and 1.035 on a random sample should be considered normal if kidney function is normal. Any measurement below 1.007 to 1.010 indicates hydration and any measurement above it indicates relative dehydration. Urine having a specific gravity over 1.035 is either contaminated, contains very high levels of glucose, or the patient may have recently received high density radiopaque dyes intravenously for radiographic studies or low molecular weight dextran solutions.
Protein
While the dipstick test has a portein measurement, more elaborate tests for urine protein should be performed since cells suspended in normal urine can produce a false high estimation of protein. Normal total protein excretion does not usually exceed 150 mg/24 hours or 10 mg/100 ml in any single specimen. More than 150 mg/day is considered proteinuria. Proteinuria greater than 3.5 gm/24 hours is severe and indicates the nephrotic syndrome. Dipsticks detect protein by production of color with an indicator dye, Bromphenol blue, which is most sensitive to albumin but detects globulins and Bence-Jones protein poorly. Precipitation by heat is a better semiquantitative method, but overall, it is not a highly sensitive test. The sulfosalicylic acid test is a more sensitive precipitation test. It can detect albumin, globulins, and Bence-Jones protein at low concentrations. "Trace" protein is equivalent to 10 mg/100 ml or about 150 mg/24 hours (the upper limit of normal). 1+ corresponds to about 200-500 mg/24 hours; 2+ to 0.5-1.5 gm/24 hours, a 3+ to 2-5 gm/24 hours, and a 4+ represents 7 gm/24 hours or greater.
Glucose
Glycosuria (excess sugar in urine) generally means diabetes mellitus.
Ketones
Ketones (acetone, aceotacetic acid, beta-hydroxybutyric acid) may be present in diabetic ketosis or other forms of calorie deprivation (e.g. starvation). Ketones are easily detected using either dipsticks or test tablets containing sodium nitroprusside.
Nitrite
A positive nitrite test indicates that bacteria may be present in significant numbers. Gram negative rods such as E. coli are more likely to give a positive test.
Leukocyte Esterase
A positive leukocyte esterase test results from the presence of white blood cells either as whole cells or as destroyed cells. A negative leukocyte esterase test means that an infection is unlikely. Without additional evidence there is no need for culture.
http://www.medical-library.net/urinalysis_interpretation.html
Urinalysis vs Urine FEME
Are they different?
Urinalysis
Urinalysis consists of 3 parts:-
1) Direct visual observation or inspection of urine
2) Urine dipstick test
3) Urine FEME / Microscopic Urinalysis
Observation of Urine
Normal, fresh urine is clear and pale to dark yellow or amber in color. What is considered as abnormal appearance of urine?
http://www.medical-library.net/urinalysis_interpretation.html
Urine Dipstick Test
The dipstick yields valuable information which is available by direct observation after brief immersion of the urine specimen.
Medical Library: "Urinalysis_interpretation."
Medicine Newbie: "Urine FEME microscopic urinalysis."

Urine FEME / Microscopic Urinalysis
FEME stands for Full Examination, Microscopic Examination. Urine FEME is also referred to as Microscopic Urinalysis. How is it done?
http://www.medical-library.net/urinalysis_interpretation.html
Case Study
http://www.medhelp.org/posts/Urology/urine-FEME/show/599838
Student's Notes
http://jacknaimsnotes.blogspot.com/2009/03/blood-in-urine.html
PowerPoints
http://slideplayer.com/search/urinalysis/
http://slideplayer.com/slide/2649063/#
http://slideplayer.com/slide/4062490/
Urinalysis
Urinalysis consists of 3 parts:-
1) Direct visual observation or inspection of urine
2) Urine dipstick test
3) Urine FEME / Microscopic Urinalysis
Observation of Urine
Normal, fresh urine is clear and pale to dark yellow or amber in color. What is considered as abnormal appearance of urine?
http://www.medical-library.net/urinalysis_interpretation.html
Urine Dipstick Test
The dipstick yields valuable information which is available by direct observation after brief immersion of the urine specimen.
Medical Library: "Urinalysis_interpretation."
Medicine Newbie: "Urine FEME microscopic urinalysis."

Urine FEME / Microscopic Urinalysis
FEME stands for Full Examination, Microscopic Examination. Urine FEME is also referred to as Microscopic Urinalysis. How is it done?
http://www.medical-library.net/urinalysis_interpretation.html
Case Study
http://www.medhelp.org/posts/Urology/urine-FEME/show/599838
Student's Notes
http://jacknaimsnotes.blogspot.com/2009/03/blood-in-urine.html
PowerPoints
http://slideplayer.com/search/urinalysis/
http://slideplayer.com/slide/2649063/#
http://slideplayer.com/slide/4062490/
Wednesday, 23 December 2009
Kitchen Table Medicine
You are what you eat!!!!
How often do you actually think about the fact that the nutrients contained in the food you eat are what become your skin, your lungs, even your heart, and every other part of your body?!
http://www.kitchentablemedicine.com/
Monday, 21 December 2009
Health Access
Equal access
Do you agree that all patients should be entitled to equal access to healthcare whatever their lifestyle choices?
Source: The Biopsy Report
http://biopsy.wordpress.com/2009/03/26/health-access/
NowClinic
The Virtual Visit May Expand Access to Doctors
OptumHealth, a division of UnitedHealth Group, the nation’s largest health insurer, plans to offer NowClinic, a service that connects patients and doctors using video chat, nationwide next year. It is introducing it state by state, starting with Texas, but not without resistance from state medical associations.OptumHealth believes NowClinic will improve health care by ameliorating some of the stresses on the system today, like wasted time dealing with appointments and insurance claims, a shortage of primary care physicians and limited access to care for many patients.
But some doctors worry that the quality of care that patients receive will suffer if physicians neglect one of the most basic elements of health care: a physical exam.
Q: Why is a physical exam important?
Saturday, 19 December 2009
Sunday, 6 December 2009
Saturday, 5 December 2009
ApoE Polymorphism
This Article
Abstract
Full Text (PDF)
Pubmed/NCBI databases
Gene
GEO Profiles
HomoloGene
UniGene
APOE4 and TBI
APOE4 Gene and outcome of TBI
For the past ten years research has shown, then not shown, an association between comparatively worse outcome in patients with TBI who harbor the APOE4 gene. A meta-analysis (Zhou, W., et al. 2008) showed that the APOE4 gene was significantly associated with poor outcome of TBI six-months after injury, but was not associated with the initial severity of brain injury following TBI. There are many difficulties in showing this in the litigation context, since genetic testing for this purpose is not well received by treating physicians and many facilities are unwilling to do this type of genetic testing. However, brain injury litigators need to keep trying to screen for this, especially in cases where the patient has a comparatively bad outcome which is being contested by the insurance company. Source: http://www.braininjury.com/research-archive.html
For the past ten years research has shown, then not shown, an association between comparatively worse outcome in patients with TBI who harbor the APOE4 gene. A meta-analysis (Zhou, W., et al. 2008) showed that the APOE4 gene was significantly associated with poor outcome of TBI six-months after injury, but was not associated with the initial severity of brain injury following TBI. There are many difficulties in showing this in the litigation context, since genetic testing for this purpose is not well received by treating physicians and many facilities are unwilling to do this type of genetic testing. However, brain injury litigators need to keep trying to screen for this, especially in cases where the patient has a comparatively bad outcome which is being contested by the insurance company. Source: http://www.braininjury.com/research-archive.html
Sunday, 20 September 2009
Stroke & Articulation Error
Multimedia Speech Pathology
Pelat or telor (Malay/Bahasa Malaysia, pelat; Kelantan, telor, kecek telor) is articulation error. It is not due to stroke or brain injury. It can be congenital (present at birth) or acquired (after birth). It can arise from articulators mechanism, which involve muscles of the tongue, palates (soft & hard palates)(Malay lelangit, langit-langit), labia (lips; Malay bibir), jaw and aevolar ridge (Malay hujung langit-langit berhampiran gigi).
Dysarthria is a speech problem. Possible causes are stroke or brain injury (fall affecting the head, shot in the head, concussion, hit on the head by foregin object, etc). It involves 5 components - respiration/breathing, resonance, phonation, articulation and ______.
Aphasia is resultant from stroke or brain injury. It is an acquired speech & language disorder.
Speech apraxia is the inability to reproduce sounds after hearing them. It involves voluntary (volitional) and involuntary (involitional) conditions. It is a processing problem.
More at www.mmsp.com.au

Tuesday, 8 September 2009
Diastolic heart failure and pulmonary hypertension
Heart and lung involvement

Figure 1 – Severe left ventricular hypertrophy and grade 1 diastolic heart failure are revealed by echocardiography and Doppler ultrasonography. The apical 4-chamber view shows a thickened left ventricular wall and enlarged left atrium (A). Doppler evaluation shows impaired early diastolic relaxation (E wave) and vigorous atrial contraction (A wave) resulting in an E/A ratio of less than 0.75, which signifies early reduced left ventricular compliance (B). A normal E/A ratio is greater than 1.5, since most of the diastolic filling occurs early in a compliant left ventricle with the atrial component contributing a smaller volume at a lower velocity. (LV, left ventricle; LA, left atrium.)

Heart failure with normal ejection fraction (HFNEF) contributes to the largest number of cases of pulmonary hypertension (PH) in the elderly. Studies have shown that isolated HFNEF is present in 44% to 60% of patients with heart failure.20,21 In contrast to systolic dysfunction, HFNEF results from impaired myocardial relaxation resulting in decreased compliance and impairment of diastolic ventricular filling; the problem is not with ventricular contraction but rather with diastolic relaxation.
The most common causes of HFNEF are coronary artery disease, hypertension, aging, obesity, and aortic stenosis. The diagnosis is based on the presence of heart failure symptoms in the absence of depressed ejection fraction. An echocardiogram with Doppler studies can be useful in diagnosing diastolic dysfunction. The E/A ratio, in which E denotes the early peak mitral diastolic inflow velocity and A denotes the late diastolic peak mitral inflow velocity, can be useful.
Under normal conditions, E is greater than A and the E/A ratio is approximately 1.5. In early diastolic dysfunction, relaxation is impaired and there is vigorous atrial contraction, resulting in an E/A ratio of less than 0.75 (Figure 1). As the disease progresses, left ventricular (LV) compliance is reduced further, which increases early LV filling despite impaired relaxation, resulting in pseudonormalization of the E/A ratio to 1.5. In severe diastolic dysfunction, the E/A ratio is greater than 2 as a result of the LV filling occurring primarily in early diastole.22Source: Pulmonary hypertension in the elderly, part 2: Treatment
{kind=link}
http://jrd.consultantlive.com/display/article/1145425/1405017?pageNumber=6
Left ventricular hypertrophy and diastolic dysfunction
Kidney patients and their heart problems
Patients with chronic renal failure (CRF) on maintenance hemodialysis (HD) experience a series of metabolic and hemodynamic abnormalities that predispose to anatomic and functional change in myocardial performance1. Thus, left ventricular (LV) hypertrophy, a geometric change independently predictive of mortality2,3, is usually accompanied by diastolic dysfunction. Left ventricular systolic dysfunction seems to be less frequent4,5, although it also adds prognostic value6.
Patients with chronic renal failure (CRF) on maintenance hemodialysis (HD) experience a series of metabolic and hemodynamic abnormalities that predispose to anatomic and functional change in myocardial performance1. Thus, left ventricular (LV) hypertrophy, a geometric change independently predictive of mortality2,3, is usually accompanied by diastolic dysfunction. Left ventricular systolic dysfunction seems to be less frequent4,5, although it also adds prognostic value6.
REFERENCES
1. Alpert MA. Cardiac performance and morphology in end-stage renal disease. Am J Med Sci. 2003; 325: 168-78. [ Links ]
2. Foley RN, Parfrey PS, Harnett JD, Kent GM, Murray DC, Barre PE. The prognostic importance of left ventricular geometry in uremic cardiomyopathy. J Am Soc Nephrol. 1995; 5: 2024-31. [ Links ]
3. London GM. Cardiovascular disease in chronic renal failure: pathophysiologic aspects. Semin Dial. 2003; 16: 85-94. [ Links ]
4. Sarnak MJ. Cardiovascular complications in chronic kidney disease. Am J Kidney Dis. 2003; 41: 11-7. [ Links ]
5. London GM. Left ventricular alterations and end-stage renal disease. Nephrol Dial Transplant. 2002; 17 Suppl 1: 29-36. [ Links ]
6. Sarnak MJ, Levey AS, Schoolwerth AC, et al. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation 2003; 108: 2154-69. [ Links ]Grade 2 diastolic dysfunction
What is "grade 2 diastolic dysfunction"? Serious or not?
External links
http://fighttexastickets.com/picsntqh/diastolic-dysfunction-echocardiography
http://www.medscape.com/viewarticle/504948_6
http://www.docstoc.com/docs/100781766/Diastolic-Dysfunction-EchoCardiography-is-the-key
http://korhelypub.hu/admin/diastolic-dysfunction
http://trialx.com/curebyte/2011/07/07/heart-failure-diastolic-photos-and-a-listing-of-clinical-trials/
http://epdatabank.cardiostim.com/search_slide/results/taxonomy%3A23?page=2
http://www.news-medical.net/health/Diastolic-Dysfunction-Diagnosis.aspx
http://www.medhelp.org/posts/Heart-Disease/What-is-diastolic-dysfunction-grade-2/show/1670285
http://www.uptodate.com/contents/treatment-and-prognosis-of-diastolic-heart-failure
http://www.mhprofessional.com/downloads/academic/0071746269/Ch016_001-005.pdf
There are four basic Echocardiographic patterns of diastolic heart failure, graded I to IV.
Grade I diastolic dysfunction is the mildest form and is called an abnormal relaxation pattern. On the mitral inflow Doppler echocardiogram, there is reversal of the normal E/A ratio. This pattern may develop normally with age in some patients and many grade I patients will not have any clinical signs or symptoms of heart failure.
Grade II diastolic dysfunction is called pseudonormal filling dynamics. This is considered moderate diastolic dysfunction and is associated with elevated left atrial filling pressures. These patients more commonly have symptoms of heart failure and many have left atrial enlargement due to the elevated pressures in the left heart.
Grade III and IV diastolic dysfunction are called restrictive filling dynamics. These are both severe forms of diastolic dysfunction and patients tend to have advanced heart failure symptoms.
Class III diastolic dysfunction patients will demonstrate reversal of their diastolic abnormalities on echocardiogram when they perform the Valsalva maneuver and are called reversible restrictive diastolic dysfunction.
Class IV diastolic dysfunction patients will not demonstrate reversibility of their echocardiogram abnormalities and are therefore called fixed restrictive diastolic dysfunction. The presence of either class III and IV diastolic dysfunction is associated with a significantly worse prognosis. These patients will have left atrial enlargement and many will have a reduced left ventricular ejection fraction indicating a combination of systolic and diastolic dysfunction. - Wikipedia
Grade I diastolic dysfunction is the mildest form and is called an abnormal relaxation pattern. On the mitral inflow Doppler echocardiogram, there is reversal of the normal E/A ratio. This pattern may develop normally with age in some patients and many grade I patients will not have any clinical signs or symptoms of heart failure.
Grade II diastolic dysfunction is called pseudonormal filling dynamics. This is considered moderate diastolic dysfunction and is associated with elevated left atrial filling pressures. These patients more commonly have symptoms of heart failure and many have left atrial enlargement due to the elevated pressures in the left heart.
Grade III and IV diastolic dysfunction are called restrictive filling dynamics. These are both severe forms of diastolic dysfunction and patients tend to have advanced heart failure symptoms.
Class III diastolic dysfunction patients will demonstrate reversal of their diastolic abnormalities on echocardiogram when they perform the Valsalva maneuver and are called reversible restrictive diastolic dysfunction.
Class IV diastolic dysfunction patients will not demonstrate reversibility of their echocardiogram abnormalities and are therefore called fixed restrictive diastolic dysfunction. The presence of either class III and IV diastolic dysfunction is associated with a significantly worse prognosis. These patients will have left atrial enlargement and many will have a reduced left ventricular ejection fraction indicating a combination of systolic and diastolic dysfunction. - Wikipedia
 |
| http://www.mhprofessional.com/downloads/academic/0071746269/Ch016_001-005.pdf |
External links
http://fighttexastickets.com/picsntqh/diastolic-dysfunction-echocardiography
http://www.medscape.com/viewarticle/504948_6
http://www.docstoc.com/docs/100781766/Diastolic-Dysfunction-EchoCardiography-is-the-key
http://korhelypub.hu/admin/diastolic-dysfunction
http://trialx.com/curebyte/2011/07/07/heart-failure-diastolic-photos-and-a-listing-of-clinical-trials/
http://epdatabank.cardiostim.com/search_slide/results/taxonomy%3A23?page=2
http://www.news-medical.net/health/Diastolic-Dysfunction-Diagnosis.aspx
http://www.medhelp.org/posts/Heart-Disease/What-is-diastolic-dysfunction-grade-2/show/1670285
http://www.uptodate.com/contents/treatment-and-prognosis-of-diastolic-heart-failure
http://www.mhprofessional.com/downloads/academic/0071746269/Ch016_001-005.pdf
Monday, 24 August 2009
Friday, 21 August 2009
Energy Metabolism in Muscle

SGD 24-25 August 2009, Year 1 Medicine, Musculoskeletal Block
SGD 23-24 October 2013, Year 1 Medicine, Musculoskeletal Block
Topics covered:
- Energy sources for muscle contraction
- Aerobic and anaerobic pathways for energy production in muscle cells
- # of ATP produced in glucose catabolism
- Reactions of glycolysis that use or produce energy (2 ATP-utilizing reactions & 3 energy-producing reactions - 2 NADH, 2 ATP, 2 ATP)
- Severe muscular exercise and plasma lactate level increase
- Cori cycle and its importance in muscle metabolism
- Glucose-alanine cycle and its importance in muscle metabolism
- Reactions of beta-oxidation that use or produce energy (1 ATP-utilising reaction & 2 energy-producing reactions - 1 FADH2, 1 NADH)
- Products of 1 cycle of beta-oxidation
- # of ATP produced by oxidation of each NADH and FADH2 in ETC
- Calculation of net ATP produced from oxidation of 1 palmitic acid (C16:0)
- Citric acid cycle (Krebs cycle or TCA cycle) - where it occurs and # of energy-producing substances formed (mitochondrial matrix; 3 NADH, 1 FADH2, 1 GTP)
- Why TCA cycle is an amphibolic pathway (catabolic - oxidation of acetyl CoA, anabolic - TCA intermediates used for biochemical anabolic pathways)
- Why TCA cycle is an aerobic pathway
- Chemiosmotic theory of oxidative phosphorylation
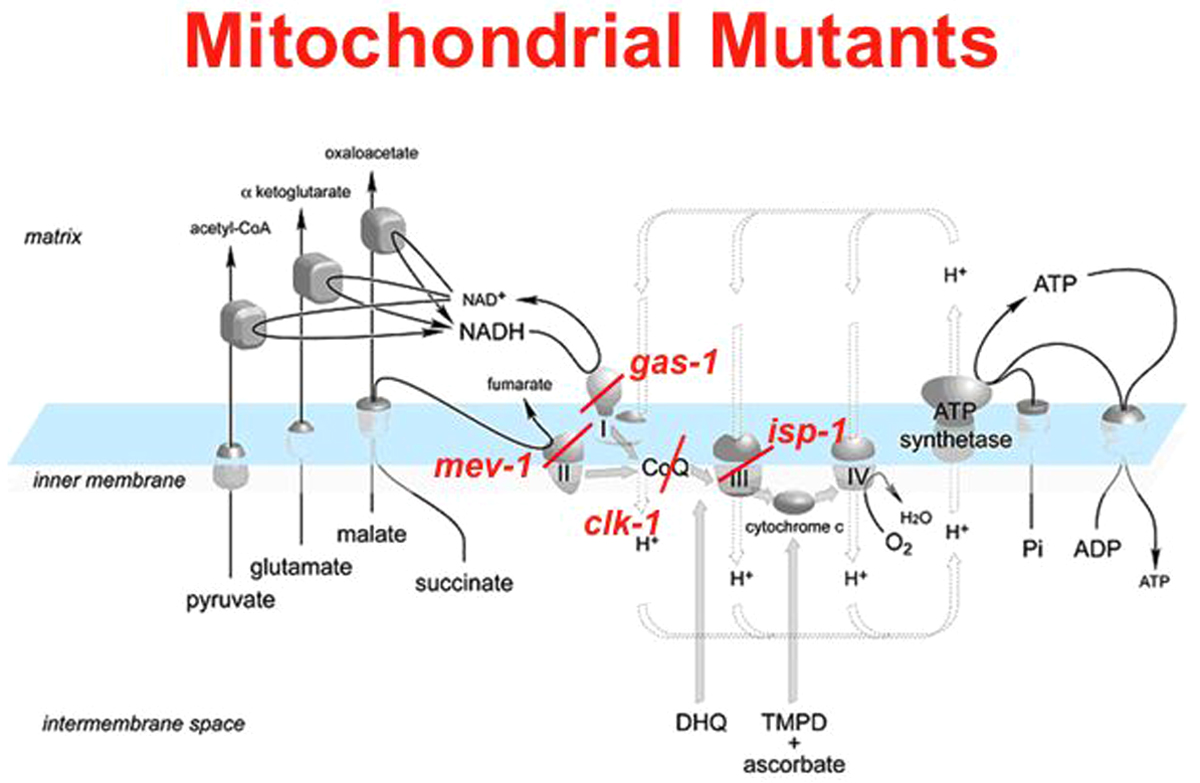
- Inhibitors and uncouplers of ETC
- Why impairment of ETC causes lactic acidosis
When the respiratory chain is blocked, pyruvate accumulates outside the mitochondria, and when too much pyruvate has accumulated, the cells start to convert it to lactic acid. Many patients with mitochondrial disease have lactic acidosis.
Inhibitors of ETC & DNA mutations cause increased NADH --> increased NADH/NAD+ ratio --> inhibition of PDH --> pyruvate cannot be converted to acetyl CoA --> conversion of pyruvate to lactate --> lactic acidosis
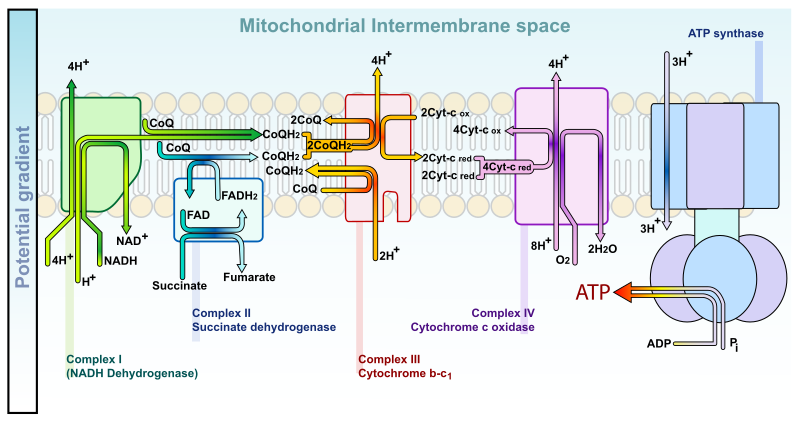
Mitochondrial DNA (mtDNA) encodes 13 subunits of ETC complexes
Nuclear DNA (nDNA) encodes >70 subunits of proteins in oxidative phosphorylation
Cori cycle
The Cori cycle involves the utilization of lactate which is produced by anaerobic glycolysis in non-hepatic tissues such as myocytes (muscle cells) and erythrocytes (red blood cells) as carbon source for hepatic gluconeogenesis. Liver then converts the lactate back into glucose for use by non-hepatic tissues. The gluconeogenic part of Cori cycle utilizes ATP (net consumer of energy, uses an extra 4 ATP) and the Cori cycle canot be sustained indefinitely.
Elimination of nitrogenous wastes
Why does the body make nitrogenous wastes? How does the body process nitrogenous wastes? The body processes nitrogenous wastes in 4 ways - 1) Glutamine, 2) Transamination, 3) Deamination, and 4) Urea. What is the role of glutamine in nitrogenous waste transport? Transamination is converting one amino acid to another. Deamination is removing the amine from an amino acid. Example of transamination and deamination is the glucose-alanine cycle. Urea synthesis occurs in the liver.
Cellular respiration
Cellular respiration is the process in which an organism breaks down fuel (glucose, glycogen, protein, lipids) to capture energy in a usable form (ATP).
Phosphorylation and dephosphorylation
When a phosphate (P) is passed from ATP to another molecule, that molecule gains enegry; this is an endergonic (energy storage) reaction. Likewise, when that phosphate is removed, both energy and heat are given off (an exergonic reaction), and the molecule contains less energy than before.
See diagrams here:
- Glycolysis, Glycolysis
- ATP yield from glucose
- TCA cycle
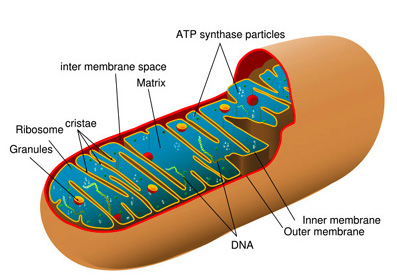
- Mitochondrion, Mitochondrion
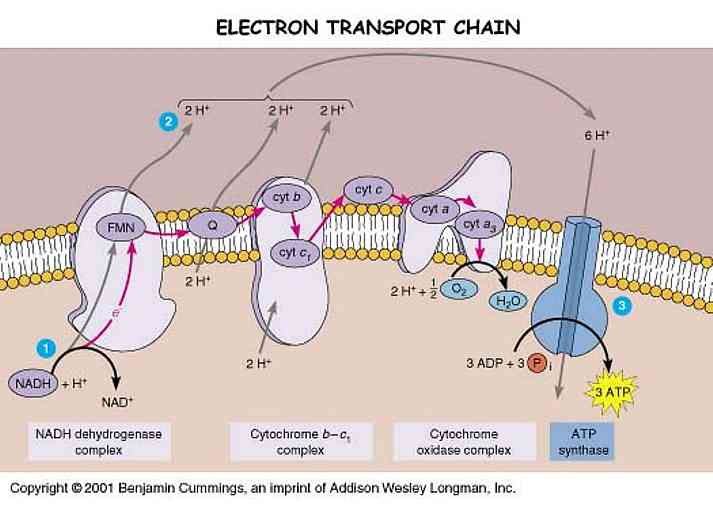
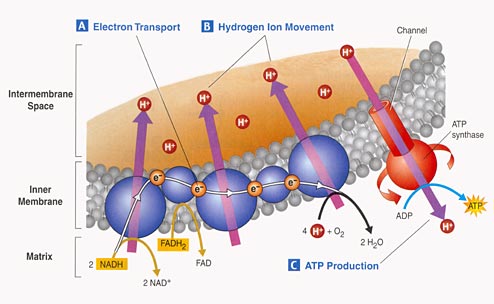
- ETC, ETC, ETC, ETC, ETC, ETC, ETC
- Oxidative phosphorylation
- Cori cycle, Cori cycle
- Gluconeogenesis, lactate and Cori cycle
- Glucose-alanine cycle, Glucose-alanine cycle
- beta-Oxidation
- Oxidation of palmitate (& everything else about lipids)
- Why minus 2 ATP for palmitate oxidation?
- Chemiosmotic theory
- Mitochondria, ETC and chemiosmotic theory
- Mitochondrial proton leak
- Inhibitors & uncouplers of ETC, Uncouplers of ETC
- Antimicrobials
- Lactic acidosis
- mDNA and nDNA mutations involving ETC complexes and oxidative phosphorylation, nuclear gene mutations, mitochondrial mutants
- Mitochondrial disease, Mitochondrial disease
- Cellular respiration
- Aerobic Energy System
- Cellular Respiration - Harvesting Chemical Energy (very good)
- Cell Biology - Endomembrane system, protein sorting and membrane trafficking (lots of diagrams)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
- Metabolism - all chemical reactions
- Anabolic reactions - synthesis; catabolic reactions - breakdown
- Phosphorylation - add P to a molecule to active/deactivate it; priming
- Processing of energy-containing nutrients - 3 stages: 1) Digestion, 2) Anabolism/catabolism, and 3) Oxidative breakdown
- Oxidation-Reduction (redox) reactions - 1) two reactions paired/always coupled, 2) electrons lost/gained, 3) involved coenzymes
- Coenzymes - nicotinamide adenine dinucleotide (NAD+) and flavin adenine dinucleotide (FAD)
- Mechanisms of ATP synthesis - 2 ways - 1) Substrate-level phosphorylation (SLP) - direct, and 2) Oxidative phosphorylation (OP) - Chemiosmotic processes - membrane & chemical reactions
- Carbohydrate metabolism - complete oxidation of glucose - 3 stages - 1) Glycolysis, 2) Citric acid cycle/Krebs cycle/TCA cycle, and 3) ETC/OP
- Complete oxidation of glucose: C6H12O6 + 6O2 --> 6H2O + 6CO2 + 36 ATP + heat
- Glycolysis - breakdown of glucose to pyruvate - 3 phases - 1) Sugar activation - uses ATP to make fructose 1,6-biP, 2) Sugar cleavage - fructose 1,6-biP --> glyceraldehyde 3-P & dihydroxyacetone P, 3) Oxidation & ATP formation - 3C sugars oxidized (NAD+ reduced) and Pi attaches to each oxidized fragment. Final products of glycolysis: 6H2O + 6CO2 + 36 ATP + heat
- Citric acid cycle/Krebs cycle/TCA cycle - fueled by pyruvic acid and free fatty acids (FFA)
- Formation of acetyl CoA - 3-step process - 1) Decarboxylation, 2) Oxidation - removal of H atoms from pyruvic acid, and 3) Formation of acetyl CoA
- Electron Transport Chain (ETC) - 1) Accepts H+, 2) Protein chain (cofactors), 3) Formation of oxygen, and 4) Release of energy - oxidative phosphorylation --> ATP
- Mechanism of Oxidative Phosphorylation - 1) H --> H+ + e-, 2) Proton pump --> proton motive force, 3) Electrons shuttled, 4) Formation of water, and 5) H+ diffuse --> ATP
http://slideplayer.com/search/Energy+Metabolism/
http://slideplayer.com/slide/4352474/
Influenza A (H1N1) Pandemic
2009 Pandemic
The at risk groups:
The at risk groups:
- People with lung disease
- People with heart disease
- People with kidney disease
- People with diabetes
- Those with immunosuppression problems either because of treatment or disease
- Patients who have had drug treatment for asthma
- Pregnant women
- Children under five
Thursday, 25 June 2009
Acid-Base 2005/2006
SlideWorld for PowerPoints
I was just Googling ACID-BASE.PPT and got to http://www.slideworld.org and came across my own PowerPoint of 2005/2006 which was downloaded 28 times! Hahaha...it feels good that others in other universities in this world are using my slides. Feels really great. I will make some more slides for the world, really beautiful teaching slides...
Tuesday, 23 June 2009
Pasangan Talasemia
Welcome PTK5 lecturers! There is nobody from Hematology this year. I have a question posed to me at my other blog on mothers (www.baiboo.com - click Malay Confinement). Here is the question:
I was hoping someone from Hematology could answer this question and we all observe what happens to the couple's kids.
Subject: Pasangan Talasemia
Assalammualaikum,
Saya H. Berumur 28 tahun .Baru berkahwin selama 6 bulan.Saya adalah penghidap Talasemia Alpha dan baru-baru ini saya mendapat tahu suami saya juga penghidap Talasemia Beta.Saya ingin mengetahui selamatkah jika saya mengandung dan anak yang bakal lahir nanti adakah akan mengidap Talasemia peringkat yang lebih teruk.Saya amat berharap Dr. dapat membantu saya.
I was hoping someone from Hematology could answer this question and we all observe what happens to the couple's kids.
Monday, 22 June 2009
Undergraduate Medicine Preparatory Programs
New students will be entering university in the 3rd week of June 2009. For this year, preparatory programs for medicine are being held at UM, MSU in Shah Alam and other places. Govt scholarships for undergraduate medicine are for attending universities in the Czech Republic, Poland and India. Students will not be sent to UK or Australia anymore. Govt scholarship bodies are still MARA & JPA. Students who go overseas using private funds to do first year medicine with the hope of applying for govt scholarships will be frustrated as this avenue has been terminated (tak dilayan). Good Luck to Farah for attending MSU on 23 June 2009. Always read al-Quran (Surah al-Mulk) and Nabi Muhammad SAW's prayers (Ma'thurat). Remember Allah always for He is Forever Knowing and Knows All. Be thankful to Allah for whatever you have. Be kind to your siblings, parents and elders. May you learn to be a humble doctor for yourself and for others. Mummy & Daddy.
Saturday, 13 June 2009
Useful programs and webpages
Author Stream, Geni, Facebook, My Space, Wizehive, Playlist, Scribd, Skype, NHINWatch, Enveluv, Medicalppt, Dia, Blogger, Huddle, Gigya, Weebly, Adrive, LinkedIn, Twitter, FreeMedicalPodcasts, Stumble Upon, Typenow, Trainingmalaysia, Studymalaysia, Evernote, YouSendIt, Fliiby, Virtuallythere, Koyote, Research Gate, medGadget, www.medic.usm.my, ernd.usm.my, HUSM PACS IW, HUSM MyRIS, MyPACS, Patientslikeme
Sunday, 31 May 2009
Video Download Managers
31 May 2009, 11.24pm - Youtube flv downloader (54.38K), 1-Click YouTube Downloader (3.25MB), Internet Download Manager, YouTube Downloader, Easiestutils Youtube Downloader 2.3.9 (1.85MB).
Friday, 29 May 2009
The Early Malay Doctors (TEMD)
This is my second book...it is a history book for Malaysians. I've just submitted my manuscript to USM Publishers on 26 May 2009. It will undergo Review. Will update at The Early Malay Doctors blogspot.
Subscribe to:
Comments (Atom)